
GASTRIC INTESTINAL METAPLASIA AND DYSPLASIA. Bogotá Endoscopy
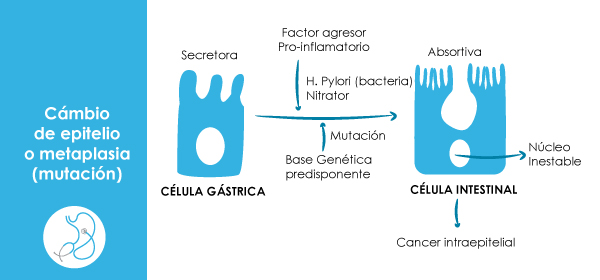
Metaplasia is the change of an epithelium with one that should not be in that mucosa, in this case the stomach which is replaced by specialized intestinal epithelium. Metaplasia is recognized as a premalignant condition that usually is a response to a stressor such as smoking, nitrous mines, high salt intake and infection with cancer-causing strains of Helicobacter pylori. Patients with more if incomplete metaplasia are at increased risk to more than 10 times of gastric cancer and can usually precede dysplasia (intraepithelial cancer).
The benefits of screening or surveillance which can be performed initially with radiographs stages of double-contrast gastrointestinal tract of high-risk populations or better performing endoscopy in that same type of population leads to finding an incidence of 11% and this can lead to early diagnosis of gastric cancer and thus in improved survival.
Patients with dysplasia of low and high grade have a high incidence of gastric cancer and the incidence of gastric cancer in the follow-up endoscopic of this type of patients was 33% to 85%, in fact the high-grade dysplasia is considered intra-epithelial cancer non-invasive and yet at this stage is capable of healing with mucosal resection. The incidence of early gastric cancer in patients with high-fat dysplasia can reach 62% in a cohort of surveillance.
Some studies suggest a low risk of cancer in patients with metaplasia, but if they also have dysplasia tracking endoscopy should be performed every 3 months with mapping biopsies during the first year when such monitoring can be spaced 2 sessions of successive biopsies show results negative.
Patients with high-grade dysplasia should undergo gastric mucosa endoscopic resection possible by the high probability of coexisting with invasive adenocarcinoma.
Biopsies of the lesser curvature mapping in high-risk patients can provide useful information to assess the risk of cancer.
If infection with Helicobacter pylori is found it must be eradicated to decrease the likelihood of gastric cancer.
When is gastric dysplasia should be practiced mapping to determine their extent and severity and take biopsies including minimal angular notch, major and minor curvature and sidewalls with an emphasis on lesser curvature. If an ulcer is found should be given treatment and make a new endoscopy 4-6 weeks Bogotá and new biopsies if dysplasia persists should be considered early gastric cancer and endoscopic mucosal resection should practice. If you are located in a polyp or lesion in a susceptible endoscopic resection should be performed mucosectomy. If the diagnosis is an area with no apparent injury is one more indication of chrome mapping endoscopy.
Bibliography
- Plazuelo MB Epplein M. Correa P.. Gastric cáncer an infectios disease. Infect Dis Clin North Am 2019, 24-853-69,vii
- CorreaO. Plazuelo MB. Wilson KT . Pathology of gastric intestinal metaplasiaclinical implivcations An J Gastroenterol 2010;105 :498-8
- WhitingJl.,Sigurdsson A. Rowlands DC, Hallissey MT. Fielding JW. The long term result of endoscopic surveillance of premalignant gastric lesions. Gut 2002; 50: 378-81
- Rokkas T., Filipe Mi., Sladen GE, Deteccion of an ancreseased indidance of early gastric cancer in patiens with intestinal metaplasia type III who are closely followedup. Gut 1991. 32:1100-3
- Srivastava A. L lauwers GY. Gastric Ephitelial dysplasia the Western perspective. Dig Liver Dis 2008, 40:641-9
Doctor. Guillermo Segundo Pérez González. . Internist Gastroenterologist. Javeriana University. Universidad del Rosario Bogotá Colombia
Leave a reply